Surgery, chemotherapy even cutting-edge immunotherapy — all failures. The cancer growing along the surface of the patient’s skin was overpowering their body’s last defenses. Traditional treatments for a typically curable skin cancer had all been unsuccessful. A clinical trial about 300 miles away and across an international border from the patient’s home in Germany was a last hope.
Across the globe in Philadelphia, researcher Andrew South, PhD, sat glued to video conference calls with collaborators at all hours, coordinating the trial and tracking the patient’s progress. This patient would be the first to enroll in a study that the team hoped could halt the cancer’s progress.
For most people, a type of skin cancer called squamous cell carcinoma is treatable, and survivable when caught early. But for this patient and thousands of others living with a condition known as recessive dystrophic epidermolysis bullosa (RDEB), commonly referred to as “butterfly disease,” the cancer is a death sentence.
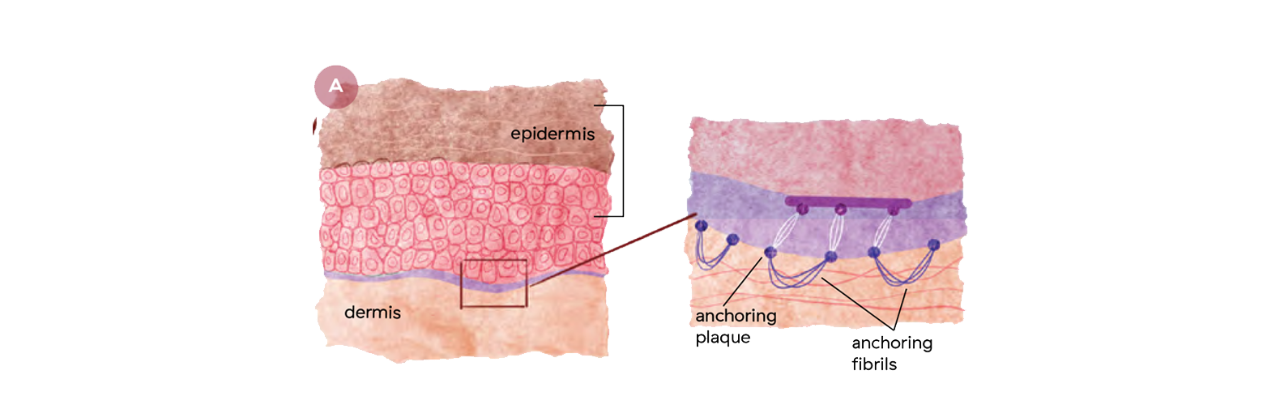
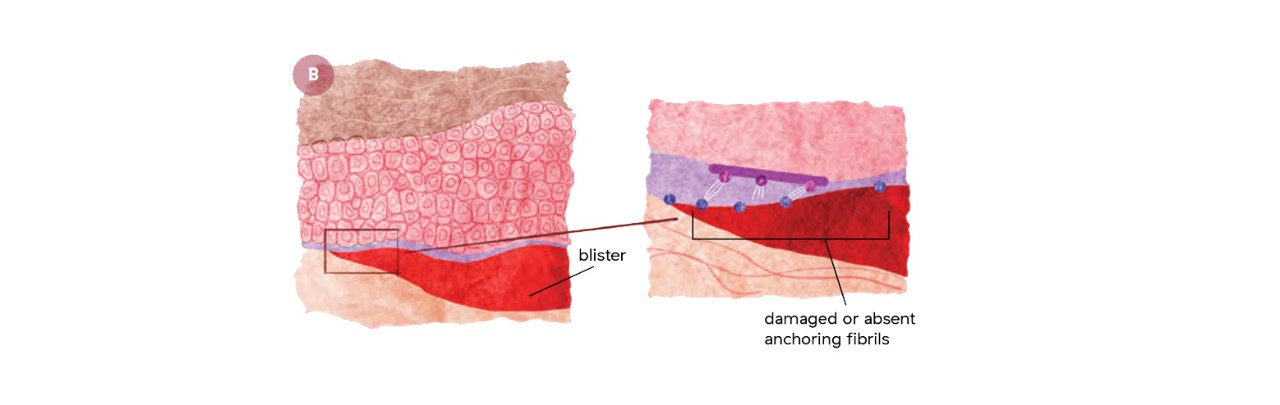
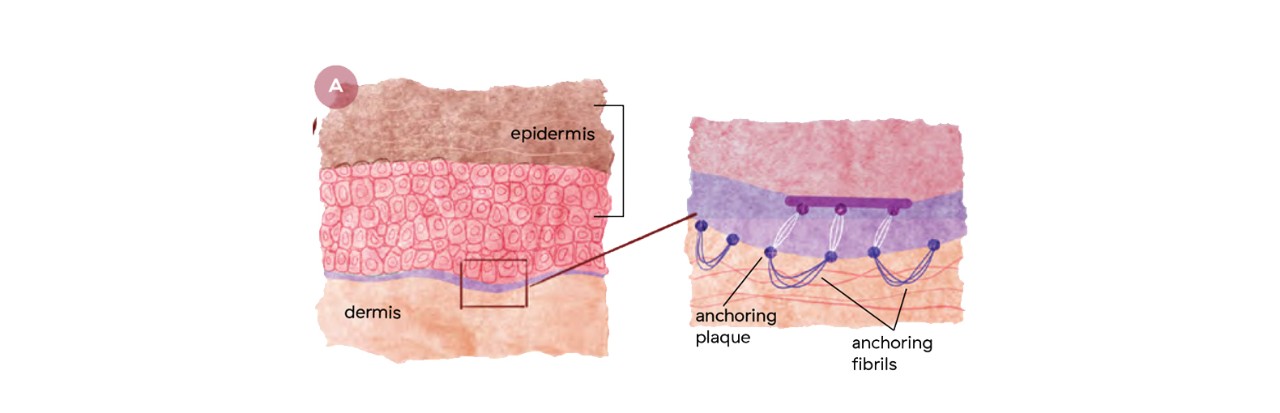
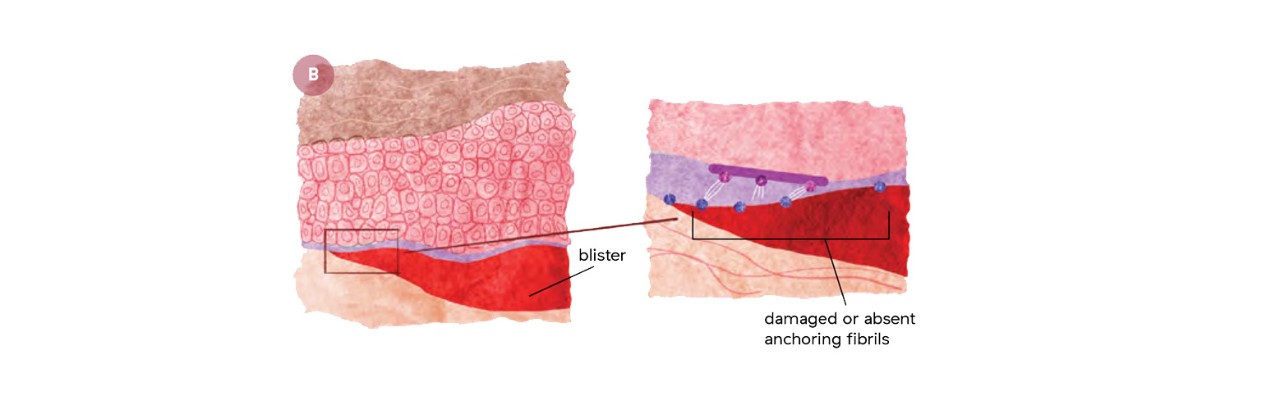
RDEB is a rare genetic condition that makes the skin incredibly fragile. Patients with RDEB do not make enough, or any, of a protein called collagen 7, that helps to hold layers of the skin together, due to mutations in a single gene. Without collagen 7, the skin cannot make anchoring fibrils, which act as the glue between the upper and lower layers of skin. As a result, the skin is so delicate the slightest touch makes these layers separate and blister. Because anchoring fibrils also help hold together layers of mucosal surfaces in the mouth, esophagus and anal sphincter, blisters in the mouth and along the esophagus make swallowing difficult. Eating may require a feeding tube and laxatives and stool softeners are helpful, and sometimes necessary, for defecation.
It is the almost constant inflammation and chronic scarring from the blisters that lead to the nearly inevitable development of skin cancer. Chronic inflammation, or persistent infection anywhere in the body can lead to cancer because inflammation damages DNA, causes cells to multiply faster and stimulates the growth of blood vessels that bring oxygen and other nutrients to the area — all factors that support cancer development. Individuals with RDEB live with chronic inflammation and often develop skin cancer within the second or third decade of life. The majority of patients do not live to celebrate their 35ᵗʰ birthdays.
“This disease is diabolical in its cruelty,” says Sharmila Collins, founder of Cure EB, a patient advocacy and funding organization, and mother to Sohana who lives with the disease. “A treatment would be a massive relief, the lifting of a death sentence.”
While progress has been made for many other cancer types, a treatment for the skin cancer in RDEB patients has evaded scientists. Many molecules can look promising in laboratory experiments, but few actually make it through clinical trials with patients, and far fewer of those become approved drugs. A decade ago, Dr. South discovered a molecule that appeared to drive skin cancer in cells derived from patients with RDEB. He didn’t know it then, but that discovery would be the first of many leading to a treatment for the disease.