04.03.23
Restoring Smell & Taste after COVID
By Shellie Wass and Karuna Meda | Illustrations by Chiara Zarmati
photographs by ©Thomas Jefferson University Photography Services
Promising results from a clinical trial to treat loss of smell provide hope to patients searching for treatment.

For as long as Nancy Damato can remember, smell and taste have been interwoven into her very being. These senses bring up memories of large Italian dinners with her family every Sunday, and the feast of the seven fishes every Christmas Eve. A self-professed foodie, she enjoys visits with her stepson who is a top chef in New York. She collects perfumes and as an avid yoga enthusiast, she enhances her practice with essential oils. “In what seemed like a nanosecond, all of this was taken away without a trace.”
Damato was one of thousands infected by the novel coronavirus during the first wave of the pandemic. She initially considered herself lucky — with mild symptoms, she continued her daily yoga routine and worked from home. But a few days into her quarantine, she realized she couldn’t smell her morning coffee or taste her food. Alarmed, she called her doctor and discovered she was experiencing a phenomenon known as anosmia.
Since the beginning of the COVID-19 pandemic, over 96 million Americans have been infected with the coronavirus. With the earliest variants of the virus, loss of smell or anosmia, was one of the first signs. Although this symptom has become less common with more recent variants like omicron, it is estimated that 27 million people are still experiencing long-term anosmia.
David Rosen, MD, an otolaryngologist at Jefferson Health, has been studying and treating anosmia for over two decades, but has never seen it at this scale. “Before COVID-19 hit, I would see one or two patients with anosmia a month,” he says. “Now I see three or four patients per day.” He has long searched for a treatment for anosmia and other smell disorders. In 2019, he and his team began investigating a tool called platelet-rich plasma (PRP), which is thought to help regenerate the cells in the nose that enable us to smell. Little did he know that just a year later, anosmia and this treatment would be thrust into the spotlight.
Damato came across an article on Dr. Rosen’s study, and it felt like a lifeline. She was told by her doctor that her senses would return after two weeks — but the time came and went, and she began desperately looking for ways to regain her senses. She reached out to Jefferson Health just in time — the clinical trial was still enrolling patients. Her and Dr. Rosen’s journey offers hope to millions of patients still looking to restore the vital sense of smell and shines a light on a condition that has long been poorly understood.
 Nancy Damato during an appointment with Dr. David Rosen.
Nancy Damato during an appointment with Dr. David Rosen.
The Underappreciated Power of Smell
The ability to smell is a complex process involving the nose and brain. It begins with odor molecules in the air passing through your nostrils and to a strip of tissue inside the nose called the olfactory epithelium. This tissue is home to millions of cells called olfactory sensory neurons, which are like taste buds of the nose. Each of these neurons has receptors that bind the odor molecules floating around. When detection happens, the neurons send an electrical signal to the brain, where it is processed into a scent that we’re able to recognize.
“The sense of smell enriches our everyday lives, helps us understand our environment and form memories,” says Nancy Rawson, PhD, the acting director of Monell Chemical Senses Center in Philadelphia. “But the role of smell in humans has been underappreciated because we are such visual and sound-oriented animals.”
Monell is a global leader in smell and taste disorders, and a long-time collaborator with Jefferson. Their connection dates back to the late 90s, when they started the Taste and Smell Clinic located in Jefferson’s Ear, Nose and Throat (ENT) Department. It was through the work of his mentor, Edmund Pribitkin, MD, with the clinic that Dr. Rosen developed a passion for smell disorders. Over the years, he has worked with Dr. Rawson and Pamela Dalton, PhD, another Monell scientist, on numerous projects to better understand how smell works at a cellular level.
Through their work, they met hundreds of patients who had lost their sense of smell to various causes — head trauma, nasal polyps, chronic sinus disease, infection and aging. They also witnessed the impact of impaired smell through their patients' stories. Dr. Dalton remembers a flight attendant who lost her sense of smell after a car crash and struggled to navigate once familiar contexts on her travels. “She knew what the Paris metro smelled like and without that context cue, she felt like she was in a completely new environment,” recalls Dr. Dalton. “It changes the way you move through the world — if you compare it to sight, colors that were once vibrant are now faded.”
The description resonates with Damato, who says it goes deeper than losing her ability to taste her coffee — she feels like she’s lost a part of herself. There are also long-term dangers, including not being able to smell smoke, gas or fire within your home. Anosmia patients are also at risk of developing depression and weight loss from losing the joy of tasting food, as the majority of flavor actually comes from aroma. Furthermore, an NIH-supported study involving 3,000 people above the age of 50 showed that those who could no longer detect or distinguish odors were four times more likely to die within five years than those with a normal sense of smell.
It’s clear that smell is important. Furthermore, impairments in smell are actually quite prevalent. In fact, before the pandemic nearly one in four Americans over the age of 40 reported some alteration in their sense of smell. But it has been challenging for researchers like Dr. Rosen and those at Monell to convince funders to invest in their work. In 2011 the joint clinic closed because funding ran out. “And then COVID-19 changed everything,” says Dr. Rosen. Suddenly, they were getting frantic calls from patients and journalists for answers — how exactly is SARS-CoV-2, the virus behind COVID-19, causing the loss of smell? And how do we treat it?
COVID-19 Sabotages Smell-Sensing Cells
With other viral infections, the loss of smell and taste is a secondary symptom that occurs due to congestion and inflammation of the nasal passages. But with COVID-19, loss of smell is one of the first signs that precedes other cold-like symptoms. This initially baffled scientists and doctors. “If you look at the noses of COVID-19 patients with a scope, they look pristine compared to other post-viral patients whose nasal passages are clearly swollen and obstructed,” says Dr. Rosen.
But a closer look at the olfactory epithelium in the nose reveals a different picture. The smell-sensing neurons are interspersed with various support cells that remove waste, provide nutrients and maintain the optimal balance of ions in the cellular environment. Researchers have found that some of these support cells are full of ACE-2 receptors, which the SARS-CoV-2 virus uses as a key to gain access into cells.
Once infected, the support cells become targets for the immune system and inflammation kicks in. Dr. Rawson says that scientists don’t yet know the exact mechanism, but they think the inflammatory cascade causes the olfactory sensory neurons to drastically reorganize their genetic material. Without the correct genetic code, the neurons can’t produce the receptors they need to detect odor molecules. This is another unique feature of COVID-19 – while other viruses like influenza and polio directly attack the sensory neurons involved in smell, SARS-CoV-2 hijacks the supporting cells the neurons depend on to function.
For some patients, this molecular mayhem resolves in a few weeks and their sense of smell returns. For others, like Damato, symptoms persist. Many questions remain unanswered about why some people are more susceptible to prolonged smell loss than others, and whether there are lasting changes in the brain. It will be at least another decade till we can fully understand the long-term impact of this scale of anosmia.
“The silver lining to this very dark cloud is that we’ve never had such a large cohort of anosmia patients at one time, and we can pinpoint the exact cause,” says Dr. Dalton. It has focused some much-needed attention on not just understanding mechanisms, but also developing treatments.
“Before COVID-19 hit, I would see one or two patients with anosmia a month. Now I see three or four patients per day.”
David Rosen, MD
The Search for a Cure
Dr. Rosen says the gold standard for patients with smell disorders is a technique called smell training. It is easy for patients to do at home and requires mindfully smelling different scents for a few minutes each day. Some recommended scents to start with include coffee, citrus, strongly scented soaps or shampoos and candles. A patient smells the same thing repeatedly while consciously reminding their brain what they’re smelling. They would think to themselves, ‘this is coffee, this is coffee…’ and once they can begin to recognize that scent, they move on to another.
Damato has made smell training part of her daily routine. When she does yoga, she lines up her different essential oils and practices smelling each to help trigger her memory. Previous evidence has shown that about 30% of patients had improved smell after performing smell training for three months. But the success can vary depending on the severity, duration and cause of the smell loss. Sticking with the exercise can also be challenging.
Since inflammation can contribute to disrupted smell, steroids in the form of nasal sprays or rinses are also prescribed. But their success in COVID-19-related anosmia is limited. There have also been some early experiments with intranasal vitamin A, which has been shown to be beneficial in other forms of smell loss. Doctors also prescribe it as a supplement, along with omega-3 and alpha-lipoic acid, which are generally anti-inflammatory and have restorative properties.
“But these treatments don’t have robust science behind them,” says Dr. Rosen. “And they’re more like band aids, so improvements, if they occur, are usually short-lived. We need something that’s actually going to repair the cellular damage.” This is where platelet-rich plasma comes in.
Treating Anosmia
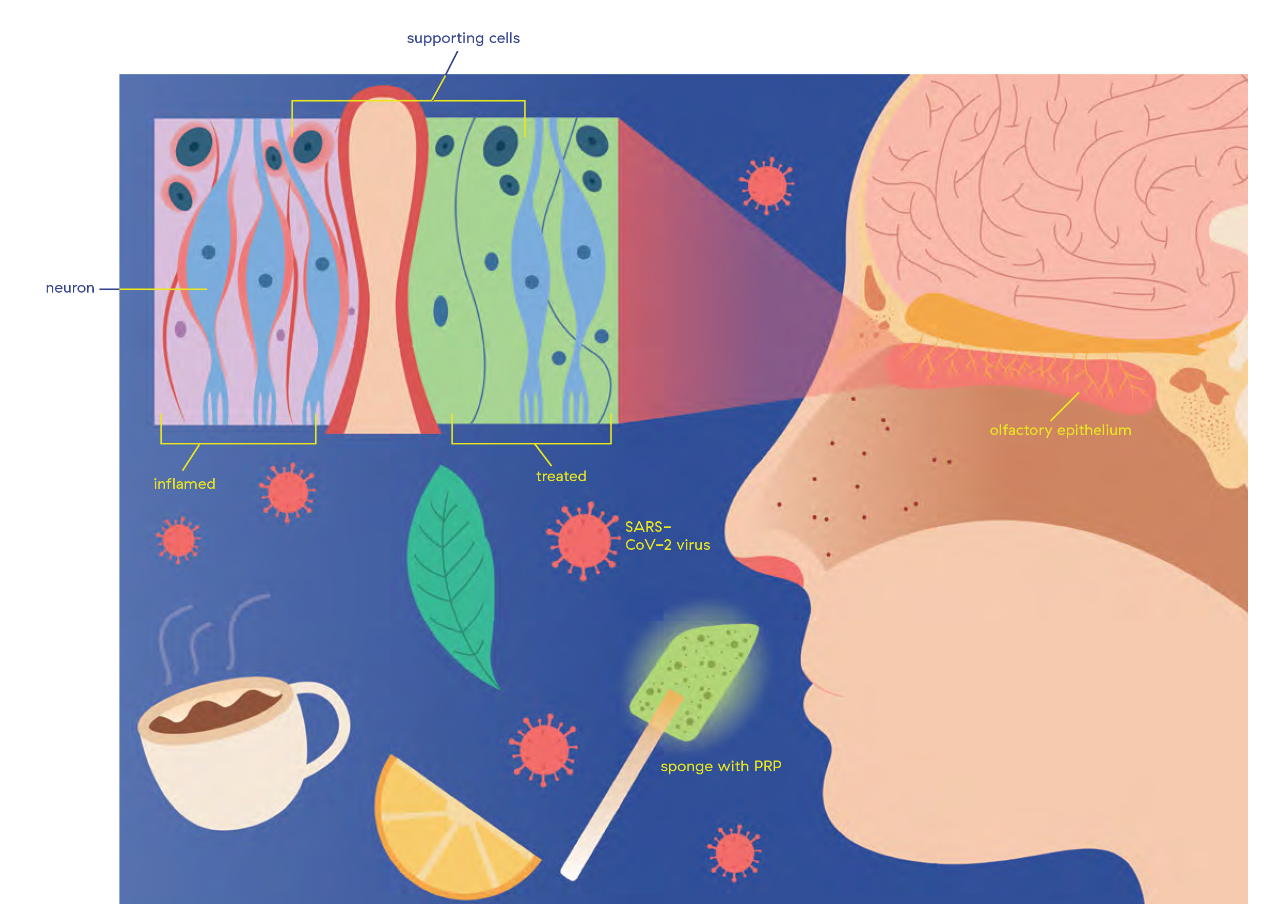
Inflamed
The SARS-CoV-2 virus enters the nostril and travels to the olfactory epithelium, where it binds to ACE-2 receptors on the supporting cells around the olfactory sensory neurons (blue), causing inflammation (in red). This in turn causes genetic changes in the neurons, hindering their ability to correctly detect smell.
Treated
After spraying a numbing agent up the nose, a dissolvable sponge saturated with platelet rich plasma or PRP is inserted using an endoscope. The sponge dissolves over time into the olfactory epithelium, where PRP is thought to regenerate damaged supporting cells (in green) and the olfactory sensory neurons’ ability to detect smell.
For a full-size version of this graphic, download the full PDF.
A Regenerative Approach
Platelet-rich plasma or PRP, as its name suggests contains platelets, a blood component known for its clotting properties. They also produce growth factors that can stimulate tissue regeneration. As a treatment, PRP is generated from a patient’s own blood, a sample of which is spun down rapidly in a centrifuge to separate the platelets from other blood cells and concentrate them within the plasma, the clear liquid portion of blood.
Dr. Rosen first became interested in PRP as a regenerative technique because of family members who had undergone injections of PRP into their joints to stave off invasive surgery for orthopedic conditions. Indeed, PRP has been successful in healing damaged tissue in conditions like back pain, and in regenerating healthy cells in scar removal and hair growth.
In 2018, Dr. Rosen came across a study where researchers injected PRP into the noses of patients with anosmia. While it was a small sample size, four out of five patients reported some improvement in their ability to smell. It was one of the first studies that had used a regenerative approach for smell disorders; Dr. Rosen wondered if he could build on this and develop a delivery system for PRP that was less invasive than an injection.
“Nasal absorption is so good that if you don’t have a way to deliver something intravenously and you need to get it into the body quickly, the nose is an effective way,” he says. A good example is the Narcan nasal spray that can save people experiencing opioid overdose.
Dr. Rosen and his team began developing a topical method, using dissolvable sponges saturated with PRP. After spraying a numbing agent up the nose, the sponges are inserted into the nasal cleft using an endoscope. The sponge dissolves over time into the olfactory epithelium, where the researchers hypothesize PRP gets to work to regenerate damaged cells.
They began testing their approach in 2019 with one patient, who showed improvement. She had lost her smell as a result of another viral illness almost three years prior. As they looked to enroll more patients, the pandemic hit, and they saw a massive uptick in interest. But it wasn’t just from COVID-19 patients — for people who had struggled with anosmia for so long due to other causes, this treatment offered renewed hope.
 Dr. Rosen and his colleague Dr. Glen D’Souza use an endoscope to guide the placement of the dissolvable sponge saturated with PRP inside Damato’s nose.
Dr. Rosen and his colleague Dr. Glen D’Souza use an endoscope to guide the placement of the dissolvable sponge saturated with PRP inside Damato’s nose.
The Promise of Platelet-Rich Plasma
Phase 1 of the clinical trial began in September 2020 with eleven patients experiencing smell loss, the majority of whom had lost their sense of smell to COVID-19. To get a baseline of their ability to smell, they underwent several types of smell tests, including the Brief Smell Identification Test™ which captures whether or not a patient was able to identify a particular scent. After this initial screening, patients had three monthly PRP treatments, and their ability to smell was tested one month after each session.
Nancy Damato joined the trial in October 2021, eight months after her initial recovery from COVID-19. She couldn’t smell anything, even if it was right under her nose, and she was unable to taste any of her food. “I felt so lost,” she remembers. “Dr. Rosen and his team were so empathetic.”
The results of their pilot trial are promising. Among those who completed a three-month course of PRP treatments, 60% experienced improvements. “This is nearly double the improvement seen with smell training, the tried-and-true treatment for smell disorders,” says Dr. Rosen. To his knowledge, it is the first and only study to date investigating the use of topical PRP treatment for smell loss.
Since ending the clinical trial, Damato has continued to see improvements. She is able to recognize scents such as lemon, rose, lavender and peppermint and can occasionally smell odors in the air. She is now able to differentiate between sweet and salty food, and can taste hints of flavors: the peppery flavor of arugula, some flavors in plain yogurt. She says her morning coffee and wine still don’t taste the way she remembers. “But it’s a huge improvement from when I first enrolled in the trial and I’m happy with my progress,” she says. “It was also so comforting to meet other patients and to know that I am not alone.”
What’s Next?
Dr. Rosen and his team hope to expand their PRP treatments to even more patients with smell disorders, and a phase 2 placebo-controlled trial is now underway. To capture additional information of patients’ baseline ability to smell, the researchers are also including the SCENTinel™ test developed by Monell. This test indicates the intensity at which patients can smell and how pleasant a scent is. “In the clinic, a patient might perform well at identifying different scents,” says Dr. Rawson. “But when they’re out in the real world, where scents are present at different intensities, they may not be able to smell as well. So this test paints a more accurate picture.”
These studies will collect more evidence for PRP as a treatment not just for COVID-19-related anosmia, but for other types of smell loss as well. “PRP is like a soup of healing agents,” says Dr. Rosen. “If it’s able to regenerate the tissue in the nose, it should have the ability to reawaken smell that has long been dormant.”
More than anything, he’s relieved that he finally has a tool to offer patients and can send them home with hope.
