04.03.23
Cancer in Butterfly Disease
By Roni Dengler | Illustrations by Greg Betza
Years of research point to a therapy to treat the life-threatening cancer of patients with a rare disorder known as butterfly disease.

Surgery, chemotherapy even cutting-edge immunotherapy — all failures. The cancer growing along the surface of the patient’s skin was overpowering their body’s last defenses. Traditional treatments for a typically curable skin cancer had all been unsuccessful. A clinical trial about 300 miles away and across an international border from the patient’s home in Germany was a last hope.
Across the globe in Philadelphia, researcher Andrew South, PhD, sat glued to video conference calls with collaborators at all hours, coordinating the trial and tracking the patient’s progress. This patient would be the first to enroll in a study that the team hoped could halt the cancer’s progress.
For most people, a type of skin cancer called squamous cell carcinoma is treatable, and survivable when caught early. But for this patient and thousands of others living with a condition known as recessive dystrophic epidermolysis bullosa (RDEB), commonly referred to as “butterfly disease,” the cancer is a death sentence.
RDEB is a rare genetic condition that makes the skin incredibly fragile. Patients with RDEB do not make enough, or any, of a protein called collagen 7, that helps to hold layers of the skin together, due to mutations in a single gene. Without collagen 7, the skin cannot make anchoring fibrils, which act as the glue between the upper and lower layers of skin. As a result, the skin is so delicate the slightest touch makes these layers separate and blister. Because anchoring fibrils also help hold together layers of mucosal surfaces in the mouth, esophagus and anal sphincter, blisters in the mouth and along the esophagus make swallowing difficult. Eating may require a feeding tube and laxatives and stool softeners are helpful, and sometimes necessary, for defecation.
It is the almost constant inflammation and chronic scarring from the blisters that lead to the nearly inevitable development of skin cancer. Chronic inflammation, or persistent infection anywhere in the body can lead to cancer because inflammation damages DNA, causes cells to multiply faster and stimulates the growth of blood vessels that bring oxygen and other nutrients to the area — all factors that support cancer development. Individuals with RDEB live with chronic inflammation and often develop skin cancer within the second or third decade of life. The majority of patients do not live to celebrate their 35ᵗʰ birthdays.
“This disease is diabolical in its cruelty,” says Sharmila Collins, founder of Cure EB, a patient advocacy and funding organization, and mother to Sohana who lives with the disease. “A treatment would be a massive relief, the lifting of a death sentence.”
While progress has been made for many other cancer types, a treatment for the skin cancer in RDEB patients has evaded scientists. Many molecules can look promising in laboratory experiments, but few actually make it through clinical trials with patients, and far fewer of those become approved drugs. A decade ago, Dr. South discovered a molecule that appeared to drive skin cancer in cells derived from patients with RDEB. He didn’t know it then, but that discovery would be the first of many leading to a treatment for the disease.
From the Lab Bench: In Search of a Target
Dr. South became interested in RDEB cancer as a newly-minted doctoral graduate in 1999. He investigated the cancer from many angles over several years, looking for something unique to RDEB that would expose a weak link in the cancer that researchers and clinicians could attack with treatment.
Dr. South and colleagues made a pivotal discovery when they studied gene expression in a type of skin cell called keratinocytes. This cell type makes up most of the outer layer of the skin and produces keratin, a protein that helps to keep hair, nails and skin strong. It is also where skin cancer takes root and begins to grow.
The researchers made four sets of comparisons: healthy and cancerous skin keratinocytes from RDEB patients, versus healthy and cancerous keratinocytes from patients with typical skin cancer induced by ultraviolet (UV) light. They were expecting to find something unique about the cancerous RDEB cells, something that would explain why the cancer is so aggressive in these patients.
But the experiment didn’t give them the results they were expecting. Cancerous keratinocytes from RDEB patients weren’t all that different than cancerous keratinocytes from patients with UV-induced skin cancer. Although surprising, the findings meant that the results could apply to any type of squamous cell carcinoma, whether or not it developed from sun exposure or RDEB.
The comparison, however, did reveal big differences between healthy keratinocytes and cancerous ones, whether or not they came from patients with RDEB or UV-induced skin cancer. There were much higher levels of about 20 genes in the cancerous cells than the healthy cells. These became his potential targets.
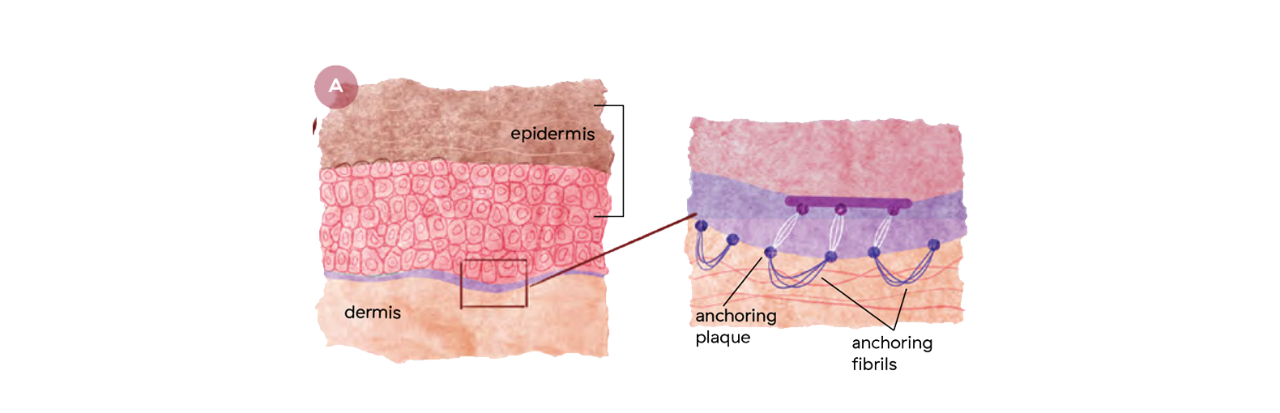 Healthy Skin: Recessive dystrophic epidermolysis bullosa (RDEB), sometimes called butterfly disease, is caused by mutations in the gene for collagen 7.
Healthy Skin: Recessive dystrophic epidermolysis bullosa (RDEB), sometimes called butterfly disease, is caused by mutations in the gene for collagen 7.
 Cancer in Patients with RDEB: The inflammation and scarring that accompanies these blisters creates an environment for skin cancer formation that is often deadly for RDEB patients.
Cancer in Patients with RDEB: The inflammation and scarring that accompanies these blisters creates an environment for skin cancer formation that is often deadly for RDEB patients.
For a full-size version of this graphic, download the full PDF.
—Catherin Gibbs, FACT Accelerated BSN Student
To pare down the list further, Dr. South and colleagues silenced the expression of each of these genes one at a time using a technology called short interfering RNA, or siRNA, to learn which ones were essential for tumor growth. siRNAs interrupt the protein-production of a gene, effectively rendering the gene non-functional, or silenced. When the researchers looked at how many cancer cells were still alive after each siRNA treatment, they saw that knocking down expression of only two of the genes they tested consistently killed a large proportion of the cancerous cells.
One of the genes, called polo-like kinase 1 (PLK1), plays a central role in helping cells multiply. Cancer cells multiply much faster than healthy cells, making PLK1 an ideal target.
Dr. South and colleagues then searched for a chemical that could do the same job as the siRNA, and would be more suitable for use in humans. One chemical they found was able to kill nearly all of the cancerous cells within three days while only slowing the growth of the healthy cells. Treating cancerous growths in mice with the chemical decreased the number of cancerous cells in as little as two weeks and dramatically shrunk the size of the tumors. Dr. South and colleagues had found their target. Now they needed to find a drug that would disable PLK1 in human patients’ cancers.
From the Lab Bench: Drug Discovery
As PLK1 plays a role in many cancers, a number of drugs that block the enzyme, also called inhibitors, were already available and in development for other diseases. In a preclinical study, Dr. South and colleagues tested six of these inhibitors in a dish on healthy and cancerous cells isolated from RDEB patients during routine diagnostic and surgical procedures. Of the six drugs they tested, one called rigosertib stood out from the rest.
Although all of the drugs that the researchers tested were good at killing cancerous cells, most of them also killed healthy cells, which might create serious side-effects for patients. That is, all of the drugs except rigosertib. “It really did nothing to the normal cells,” says Dr. South. Rigosertib was only capable of slowing the growth of healthy cells at much higher doses than required to kill the cancer cells, suggesting that if used to treat patients with RDEB cancers, rigosertib might produce fewer side effects than the other drugs.
What was more surprising, however, was how effective the drug was. Dr. South and colleagues tested rigosertib on cancerous cells isolated from 10 patients. In all 10 cases, the cancer cells died. “An efficacy of 60% is something one might think about taking into clinical trials,” says Dr. South. “Rigosertib was 100% effective.”
The researchers went on to bolster their in vitro findings in mouse models of the disease. When administered throughout the whole body, or systemically, rigosertib was very effective at stopping the cancer growth and shrinking tumors. This was another key factor in rigosertib becoming a potential treatment. RDEB patients’ cancers can spread to other parts of the body very quickly, creating metastases that can be even more difficult to treat. A drug that can be administered systemically, intravenously or with a pill for example, will target all of the cancer cells in the patient.
A year and a half after treatment with rigosertib‚ the patient remains cancer-free.
From Bench to Patient Bedside
With this promising evidence in hand, Dr. South began to secure funding to run a clinical trial. Grants from patient advocacy organizations helped to get things going, but the trial had a rocky start. The success rate for potential therapies to go from discovery to approved treatment is low. Less than 10% of potential drug treatments become approved therapies that patients can actually use. For cancer drugs, the success rate is about half that. Most drugs don’t make it past Phase I trials, where researchers assess the safety of a drug and identify side effects.
To complicate matters, rigosertib is an experimental drug that is not yet approved by the U.S. Food and Drug Administration (FDA) for any treatment. Establishing a clinical trial in the U.S. would require a complicated and long logistical process. While working to overcome these obstacles, Dr. South initially set the trial to be conducted in Europe, virtually managing the paperwork and red tape from Philadelphia. “All of that took about a year and a half just to get the contracts finished,” says Dr. South.
The trial became open to recruiting patients in Europe, at long last, in 2019. Before any patients were able to enroll, however, the novel coronavirus shut the world down. The first patient was finally able to enroll in the spring of 2021. She traveled from her home in Germany to Austria to participate in the trial. There, she checked into a hospital for a three-month stay. Clinicians administered rigosertib via an intravenous line over three days every three weeks, a task made exponentially more difficult in a patient with such delicate skin. Doctors and nurses were on constant watch for the looming threats of infection and sepsis.
Over the next months, a medical team monitored three of the primary skin-cancer lesions scarring the patient’s body. Within six months, two of the lesions showed complete remission and the third was no longer growing. Nine months after beginning treatment, all three lesions had disappeared.
“This is the outcome we’d been hoping for, after so many years,” says Dr. South.
Until now, no therapy has successfully treated this cancer in patients with RDEB. It is an unprecedented outcome for RDEB patients with advanced skin cancer.
“We are in dire need of a treatment for cancers in these patients. We’re really behind in that,” says dermatologist Neda Nikbakht, MD, PhD, a physician-scientist at Sidney Kimmel Cancer Center–Jefferson Health, who is collaborating with Dr. South to open the first U.S. trial offering a new cancer treatment to patients at Jefferson’s adult EB clinic, one of only a few of its kind in the country.
“With all the progress we made in many other cancer areas, for this group of patients, unfortunately, we don't have much to offer. This trial, and Dr. South’s discoveries, really go a long way to address these unmet needs,” she says.
Drs. South and Nikbakht have gleaned many lessons from the trial in Europe, and have been able to improve how it will be run in the U.S. The first patient in Europe, for example, had to remain in the hospital while receiving treatment, as it must be administered over 72 hours. Now, patients seen at Jefferson’s EB clinic will receive the drug as a pill. “We now have made it much easier for the patient,” says Dr. Nikbakht. “Patients will be able to receive the treatment at home.”
Stopping EB Cancer
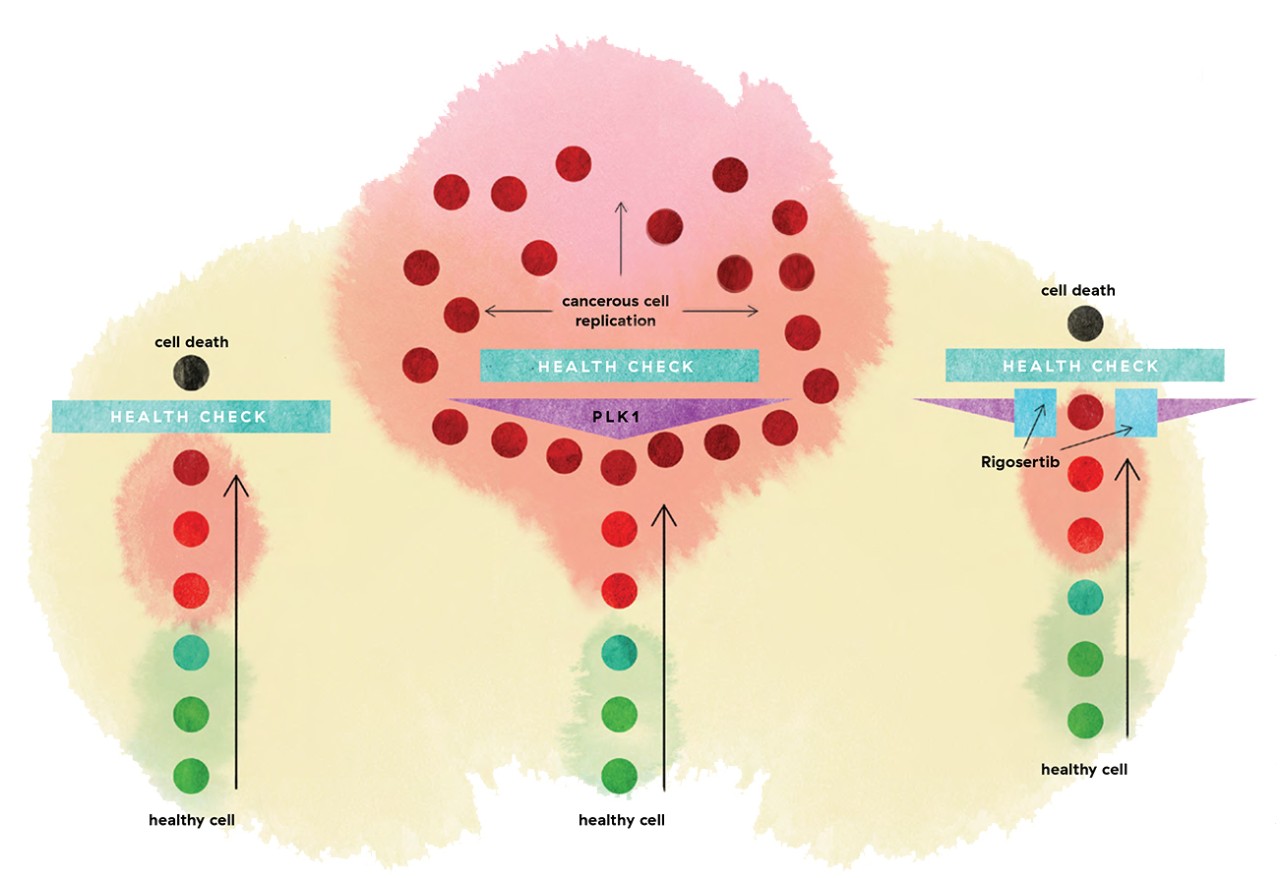
Skin cells form a tight layer of protection and also frequently reproduce to make new layers of skin. Before a skin cell can make more of itself, it has to pass through a health check to make sure it’s cleared for replication. As a healthy cell ages and accumulates damage to its DNA (progressively darker red dots), one of the first steps toward developing cancer, the cell's internal health check should prevent further replication or push the cell to self-destruct (black dots). In EB cancer (middle panel), increased amounts of a molecule called PLK1 (purple triangle) overrides the normal health check. Instead, cells with cancerous changes bypass the health check and continue to proliferate (maroon dots). Dr. South’s team found that a drug called rigosertib (blue squares) pulls back the PLK1 bypass, lets the cell identify cancerous changes, and leads those cancer cells (maroon dots) to death rather than continued growth.
For a full-size version of this graphic, download the full PDF.
 “Patient Identity” by Savannah Patterson" As part of our Research as Art contest, this piece represents the exploration of patient identity among mental health clinicians can strengthen the client-clinician relationship. This photograph explores the impact of clinician vulnerability and self-disclosure, shown by the artist’s name on the sides of medication bottles that are left open.
“Patient Identity” by Savannah Patterson" As part of our Research as Art contest, this piece represents the exploration of patient identity among mental health clinicians can strengthen the client-clinician relationship. This photograph explores the impact of clinician vulnerability and self-disclosure, shown by the artist’s name on the sides of medication bottles that are left open.
Toward Drug Approval
Drs. South and Nikbakht hope that this is only the beginning. For rigosertib to become a treatment available to patients beyond the clinical trial setting, other patients will need to have similar success as the patient in Europe.
“If we see another one or two patients with similar responses, then that will be the time to go to the FDA or the European Medicines Agency and apply for conditional approval of rigosertib,” says Dr. South. Because RDEB is a rare disease and there are no other options for RDEB patients with squamous cell carcinoma, there is potential for the agencies to approve the treatment on compassionate grounds.
Rachel Nasuti, who has enrolled in the trial at Jefferson, may be the patient to bolster such an approval. Within weeks of beginning treatment with rigosertib, Nasuti noticed a cancer lesion on her ankle had shrunk. “The wound was indented, but it’s not as much anymore,” she says. “I’m surprised at how quickly it happened. I thought I wouldn’t see results for three months.”
Nasuti has had multiple surgeries to remove areas of skin cancer over the past eight years. She has tried chemotherapy and several immunotherapy treatments, but the cancer has always returned. When she heard about the rigosertib trial at an EB conference, she was intrigued. Rigosertib wasn’t an invasive treatment and didn’t appear to have the side effects of chemotherapy.
And although surgery is the quickest, most straight-forward way to remove confirmed cancer lesions, the healing process takes a while and is painful. “You also don’t always know what lesions are cancer and what’s not,” she says. “So it’s not as targeted a treatment as rigosertib.”
An approved drug would have huge impacts for patients like Nasuti and their families. “If we had some effective therapy to kill the cancer, it will feel like freedom,” says Sharmila Collins, the founder of Cure EB. “To have that fear lifted, it means patients can go about their lives. Life might still be difficult until we find really effective treatments for RDEB, but there might be less fear that absolutely nothing can be done. I hope more than anything that this is a successful trial and will provide us a tool with which to fight the RDEB skin cancer.”
Nasuti, who lives in Michigan and drove 10 hours in each direction to enroll in the trial agrees. She is now able to continue rigosertib treatment at home between monthly visits to Jefferson. Although she is pragmatic about the possibility of the cancer returning after treatment with rigosertib, she says, “It’d be nice to live cancer free. Hopefully, rigosertib will become a treatment option for the future.”
Dr. Nikbakht and her team in the clinic are hopeful. “We are thrilled to see positive results, but we will need to rigorously evaluate outcomes over time,” she says.
Dr. South is cautiously optimistic as well. “Chances are that we will see similar responses to the drug in other patients,” he says. “But we don’t know yet, of course, and that’s why we do the research.”