Immunotherapy for human cancers is hindered, in part, by a lack of suitable target antigens. This is particularly relevant in tumors derived from mucosal tissues such as colorectal cancer, in which antigens that are sufficiently immunogenic, tumor-restricted and shared among patients are lacking, and for which conventional therapeutics are poorly efficacious. We have explored a novel class of tumor-associated antigens fulfilling these criteria by exploiting immune compartmentalization, which restricts cross-talk between systemic and mucosal immune compartments. This compartmentalization limits systemic tolerance to mucosa-restricted self-antigens and shields mucosa from systemic autoimmune responses. Thus, a novel paradigm suggests that targeting self-antigens expressed by normal mucosal tissues and by derivative neoplasms should permit effective immunotherapy against systemic metastases, without inducing autoimmunity in normal mucosa. We have explored targeting the first of these antigens, termed cancer mucosa antigens (CMAs), in animal models of metastatic cancer. Adenoviral vector vaccines were generated containing guanylyl cyclase C (Ad5-GUCY2C), expressed in normal intestinal epithelium and all primary and metastatic human colorectal cancer (CRC) specimens. Immunization elicited CD8+ T, but not CD4+ T or B, cell responses in multiple strains of mice. Moreover, responses effectively prevented the development of lung and liver CRC metastases and treated established CRC metastases in lung. This occurred in the absence of autoimmunity against normal GUCY2C-expressing tissues. These results suggest the utility of GUCY2C-specific immunotherapy for gastrointestinal malignancies, as well as the potential for CMA-targeted immunotherapy for malignancies of other mucosae such as oral, respiratory, mammary, and urogenital tissues, to treat head and neck, lung, breast, and bladder cancers, respectively. We have recently completed a Phase I clinical trial confirming the safety and immunogenicity of Ad5-GUCY2C vaccination in colorectal cancer patients. Currently, we are planning additional Phase I/II studies in gastric, esophageal, pancreatic, and colon cancer patients, with the hope that this vaccine can improve the survival of patients with these cancers.
Snook Research

1020 Locust Street
Room 368
Philadelphia, PA 19107
We study basic, translational, and clinical aspects of gastrointestinal biology and tumorigenesis. Our research projects focus on the intestinal receptor guanylyl cyclase C (GUCY2C or GCC) and its hormone ligands guanylin and uroguanylin. We have identified this hormone-receptor signaling axis as a critical pathway in intestinal homeostasis, tumor suppression and enteroendocrine signaling. We have translated those discoveries into Phase I chemoprevention studies determining the potential ability of GUCY2C hormones to prevent colorectal cancer. Moreover, we are developing novel cancer immunotherapeutics targeting GUCY2C, including vaccines and CAR-T cells. These immunotherapies could be used to treat metastatic colorectal cancer, as well as esophageal, gastric, and pancreatic cancers, which often overexpress GUCY2C.
Research Projects
Cancer Mucosa Antigens as Immunotherapeutic Targets for Metastatic Tumors
 PET/CT scans of mice with colorectal cancer metastases in the lungs and treated with control vaccine (left) or GUCY2C vaccine (right). The lungs are outlined with dashed lines. High tumor burden is see by the high FDG uptake in the control mouse, while the GUCY2C vaccinated mouse is tumor free.")
Tolerance Mechanisms Restricting GUCY2C-Specific Immunotherapy
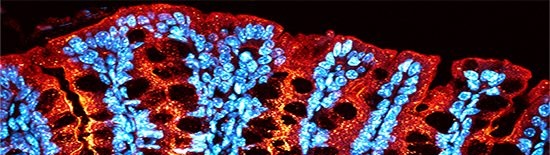
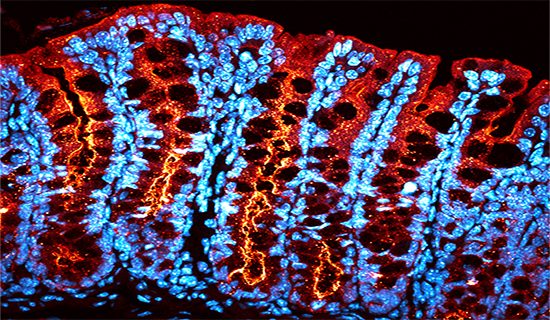
 and beta (bottom) chains of GUCY2C-specific CD4+ T-cell receptors (TCRs). TCRs identified by the sequencing are being used to create retrogenic mice to determine the mechanisms of selective CD4+ T-cell tolerance to GUCY2C.")
Immune tolerance limits immune responses to self-proteins, preventing autoimmunity and creating a significant barrier to developing cancer immunotherapeutics. Defining tolerance mechanisms for self/tumor antigens will allow for the development of new therapeutics by augmenting tolerance to treat autoimmune disorders or by inhibiting it to enhance tumor immunotherapeutic efficacy. In that context, our studies have revealed a novel tolerance mechanism limiting GUCY2C-specific immune responses and antitumor efficacy. Rather than eliminating all three adaptive immune lineages (CD4+ T, CD8+ T, and B lymphocytes), GUCY2C tolerance was characterized by selective CD4+ T cell tolerance, while CD8+ T and B cells were unaffected. Importantly, CD4+ T cells serve a critical "helper" role in immune responses, and in the absence of GUCY2C-specific CD4+ T cell responses, CD8+ T and B cell response were also inhibited. However, this creates a unique opportunity to engage latent CD8+ T and B cells, restoring antitumor immunity, through the addition of CD4+ T cell epitopes from foreign antigens (such as influenza virus). Those epitopes activate foreign-antigen-specific CD4+ T cells, which “help” GUCY2C-specific CD8+ T and B cells. That vaccination approach is being employed in our clinical trials in which patients receive a GUCY2C vaccine containing the helper epitope PADRE (Ad5-GUCY2C-PADRE). Further defining mechanism(s) underlying select CD4+ T cell tolerance to GUCY2C will create strategies for next-generation GUCY2C vaccines.
GUCY2C-Targeted Adoptive T Cell Therapy
. Mice were then treated with control or GUCY2C-specific CAR-T cells and tumor burden was monitored.")
Development of innovative paradigms beyond vaccines is needed to safely and effectively treat patients with advanced, bulky tumor metastases. While a vaccine relies on a patient's immune system to create an antigen-specific immune response, adoptive cell therapy (ACT) using engineered T cells offers unique advantages. Specifically, tolerance removes antigen-specific T cells during their maturation, limiting the number and the potency of T cells that escape tolerance and can be harnessed by vaccination. In contrast, T cells can be engineered and expanded ex vivo to produce large numbers of cells expressing receptors of high affinity, maximizing their potency. Importantly, we have shown that while GUCY2C vaccines possess antitumor activity, they are limited by tolerance, reducing their efficacy against large, established tumors. In mouse models, GUCY2C-targeted ACT is superior to GUCY2C-targeted vaccines in the context of established tumors. Similar techniques also have produced remarkable clinical successes in melanoma, neuroblastoma, and leukemia, but ACT approaches for adenocarcinomas remain limited. In that context, we are developing antigen-targeted ACT approaches which can be translated to patients with metastatic disease originating in mucosal tumors. We have shown that GUCY2C ACT employing T cells expressing chimeric antigen receptors (CARs) safely and effectively treat mice with metastatic colorectal cancer. Currently, we are developing a CAR-T cell approach that could be translated to patients with GUCY2C-expressing tumors.